1 Introduction
Prediabetes, abnormal fasting glucose (IFG) and/or abnormal glucose tolerance (IGT) is a vital state of type 2 diabetes mellitus (T2DM) (ADA, 2023). Nutritional counselling is one of the main keywords in preventing the progression of prediabetes to diabetes through promoting dietary modifications, lifestyle changes and improved metabolic markers[1]. Individualized dietary interventions have been shown to affect various biochemical parameters including fasting blood glucose (FBG), postprandial blood glucose (PPBG), glycated haemoglobin (HbA1c), lipid profiles and insulin sensitivity[2].
Structured nutritional interventions, including personalized nutrition plans, calorie restriction and behavioural modification approaches have been shown to modify the risk associated with prediabetes[3]. Multiple large trials, such as the Finnish Diabetes Prevention Study (FDPS) and the Diabetes Prevention Program (DPP), have demonstrated that lifestyle modifications, predominantly through changes in diet and physical activity, reduce the risk of T2DM[2, 4].
Recent advances support the efficacy of digitally-delivered and personalized approaches. For instance, a 2022 randomized controlled trial demonstrated that a 12-week digital nutrition intervention significantly improved HbA1c and fasting glucose in adults with prediabetes[5]. Furthermore, emerging research underscores the importance of sex-specific approaches, as metabolic responses to lifestyle changes are increasingly shown to vary by gender and menopausal status[6, 7].
Nutritional counselling focuses on teaching individuals how to plan balanced meals, control portions and distribute macronutrients. Studies have shown that both a lower total carbohydrate load and a relative dependence on complex carbohydrates with a low glycaemic index (GI) improve glycaemic control[8]. Dietary patterns such as the Mediterranean diet, which are rich in monounsaturated fatty acids (MUFA), have been associated with improved insulin sensitivity and lipid profile[9]. A randomized trial, the Diabetes Prevention Program (DPP) demonstrated that a moderate reduction in total energy intake together with an increase in physical activity reduced diabetes incidence by 58% in high-risk individuals[2].
Evidence from recent studies indicates a potentially beneficial effect of protein intake, especially from plant sources on insulin sensitivity and glycaemic control[10]. The metabolic parameters in pre-diabetic subjects are positively affected by replacing refined carbohydrates with lean protein sources and healthy fat (e.g., omega-3 fatty acids from fish)[11].
Dietary fibre intake has been linked to improved glucose and lipid regulation[12]. Diets rich in soluble fibre, FBG and LDL cholesterol concentrations in blood have been significantly decreased for pre-diabetic patients[13]. Dietary fibre increases satiety, modulates postprandial glycaemia, and promotes gut microbiota diversity which may play a role in better metabolic health[14]. A systematic review showed that a higher fibre intake has a possible protective role against T2DM, as it is associated with better glycaemic control and a lower risk of T2DM progression[15].
The results need to be maintained over the long term in order to continue the metabolic improvements. Studies prove that lifestyle-aided therapy, motivational counselling and behavioural therapies are of significant merit in improving lifestyle compliance, with or without pharmacotherapy[16]. Regular exercise, particularly when combined with dietary changes, magnifies improvements in insulin sensitivity and cardiovascular risk factors[17]. Prediabetes diet programs demonstrated to be more effective when paired with structured exercise programs, with greater improvements in Glycosylated Haemoglobin (HbA1c) and lipid profiles observed in pre-diabetic subjects randomized with dietary counselling plus structured exercise compared with control subjects receiving only dietary advice[18].
Further support for exercise as an adjunct to dietary counselling derives from a meta-analysis which showed that structured physical activity interventions reduce Glycosylated Haemoglobin (HbA1c) levels and increase insulin sensitivity[19]. In addition, other stress management techniques have been considered as complementary strategies to improve metabolic control in prediabetes[20].
Several studies point at the positive effects of dietary intervention on biochemical parameters in prediabetes. A meta-analysis conducted showed that lifestyle interventions significantly reduced Glycosylated Haemoglobin (HbA1c) and improved lipid profile in individuals with prediabetes[21]. A Structured dietary counselling was found to result in a decrease in both total cholesterol and triglycerides, key cardiovascular risk markers[22].
More recently, digital health platforms have emerged as effective vehicles for delivering structured nutritional counselling, with studies confirming that remote interventions can significantly improve glycemic parameters in prediabetic populations[23, 24].
2 Materials and Methods
2.1 Study Design and Population
This paper is prospective interventional study on the effect of nutritional counselling on biochemical parameters in pre-diabetic individuals. The study was conducted over a 12-week period and involved remote data collection and virtual interventions through a digital health platform affiliated with Ragus Healthcare Pt. Ltd. A total of 1,255 adult participants, aged 20–60 years, were recruited remotely from Ragus Healthcare’s existing client database. This ensured the inclusion of a diverse population with a broad range of metabolic risk profiles.
Inclusion Criteria: The participant was pre-diabetic adult subjects aged between 20 and 60 years Glycosylated Haemoglobin (HbA1c) 5.7–6.4% or fasting blood sugar (FBS) 100–125 mg/dl[25]. Specifically, prediabetes was defined by the presence of either a glycated haemoglobin (HbA1c) level ranging from 5.7% to 6.4%, or a fasting blood sugar (FBS) level between 100 and 125 mg/dL. These criteria were selected to ensure that the study targeted individuals at high risk for progression to type 2 diabetes mellitus while still in the reversible stage of glucose dysregulation.
Exclusion Criteria: Subjects with any known metabolic disorders, those taking steroids for autoimmune diseases, those on antidepressant medications, and those with a body mass index (BMI) greater than 35 kg/m², which is considered Obese II (high-risk obesity).
A total of 1,255 individuals were screened. Of these, 499 participants met the inclusion and exclusion criteria.
Intervention (Test) Group: The intervention group consisted of 309 participants who completed the 12-week structured nutritional counselling program. These individuals actively engaged with the assigned health coaches throughout the program and underwent both baseline and follow-up assessments. This group represents the cohort exposed to the complete duration of the structured intervention, allowing for longitudinal analysis of outcomes.
Control Group: The control group consisted of 190 participants who either declined active engagement with the intervention or demonstrated inconsistent connectivity with the assigned coaches, thereby failing to initiate or sustain participation in the structured program. While baseline data, including key clinical parameters, were available for these individuals, most did not complete the follow-up assessments due to lack of contact or failure to undergo scheduled follow-up test on Biochemical parameters.
All participants provided informed consent electronically via a secure online platform. The study protocol was approved by the institutional human ethics committee.
2.2 Biochemical Assessments
Fasting blood sugar (FBS) and glycosylated haemoglobin (Glycosylated Haemoglobin (HbA1c)) levels were estimated. Venous blood samples were collected through trained phlebotomists at home after overnight fasting. The samples were transported in controlled temperature ranges and tested in biochemistry laboratory.
Fasting blood sugar (FBS): Measured using glucose oxidase - peroxidase (GOD -POD) method[26].
Glycosylated Haemoglobin (HbA1c): HPLC (NGSP-certified method)[27].
2.3 Interventions of Nutritional Counselling
Participants were given tailored nutritional counselling based on the metabolic profiles. Counselling sessions were conducted via video calls by certified dietitians following guidelines provided by American Diabetes Association (ADA) and WHO.
The dietary changes concentrated on low-glycaemic-index foods, increased fibre, portions, and distribution of the macronutrients[1, 2]. They were advised to restrict refined carbohydrates and saturated fats, and to include primarily plant-derived proteins and healthy fats[10]. Participants were provided with structured meal plans and recipe guides and adherence was monitored via a digital dietary recall platform[28].
2.4 Physical Activity Guidelines
They were provided dietary counselling and urged participants to do 150 minutes of moderate-intensity physical activity each week[17]. Guiding principles in good practice in promoting strength / flexibility training for people with limited mobility were formulated and interventions based on resistance training and yoga were developed[20].
2.5 Study Duration and Follow-up
Participants in the study were followed over 12-week periods, measuring pre and post intervention biochemical parameters. Weekly digital check-ins monitored dietary and lifestyle changes through video consultations, messages, food plate pictures to assess the portion and balance.
2.6 Ethical Considerations
Prior approval from the Institutional Ethics Committee has been obtained for the study protocol. All participants electronically provided their written informed consent before enrolment, according to the principles stated in the Declaration of Helsinki (2013)[29].
3 Results
3.1 Reduction in Glycosylated Haemoglobin (HbA1c) by Age Group in male subjects
The effect of the nutritional intervention on Glycosylated Haemoglobin (HbA1c) and fasting blood sugar (FBS) levels differed by age and gender. The study found the most pronounced glycaemic effects among younger adults, likely reflecting greater metabolic flexibility and compliance with nutritional counselling[30]. This result is consistent with findings that early lifestyle interventions in prediabetes reduce the risk of diabetes by 58%[25]. The gender differences could reflect hormonal effects on insulin sensitivity in younger females[31].
Effects of dietary intervention on HbA1c also differed among male subjects according to age. Age and sex group specific reductions in HbA1c were significant however the greatest reduction was observed in younger males (20–30 years) across the board. Particularly, in that group, the HbA1c level was decreased by 0.3% (from 6.1% to 5.8%). This is in line with data which has demonstrated that lifestyle diets in those with prediabetes can reduce the risk of developing type 2 diabetes by 58%[25].
Despite a progressive decline in Glycosylated Haemoglobin (HbA1c) with increasing age across all age groups, the youngest male (20-30 years) had the greatest reduction (0.3% decrease from 6.1% to 5.8%). The smaller reduction in Glycosylated Haemoglobin (HbA1c) among the individuals might be indicative of developing insulin resistance in this age group of 30-40 years.
In older men (40-50 and 50-60 years), the reduction in Glycosylated Haemoglobin (HbA1c) is smaller (0.2%), possibly due to the age-dependent decline in pancreatic β-cell function and increased insulin resistance[32]. The slower Glycosylated Haemoglobin (HbA1c) reducing activity of the two (40-50) and (50-60) groups also show with the increasing age higher groups shows less Glycosylated Haemoglobin (HbA1c) reducing activity which favours the evidence of progressive β-cell dysfunction among elderly individuals[33].
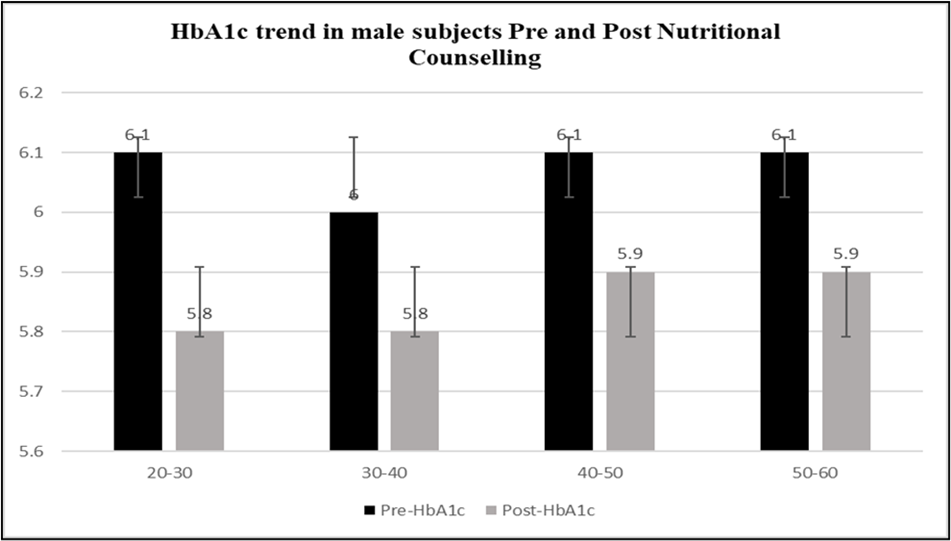
Note: This figure presents the pre- and post-intervention Glycosylated Haemoglobin (HbA1c) values across different age groups in male subjects. Error bars represent standard deviation.
3.2 Fasting Blood Sugar (FBS) changes in male subjects
Among all the age groups, the levels of FBS decreased, the most noticeable being in the case of the 40–50 years (8.4 mg/dL, from 104.2 mg/dL to 95.8 mg/dL). This is supported by research indicating that midlife men with insulin resistance respond best to lifestyle interventions[34]. The 20–30 years group demonstrated a relatively lesser decrease in FBS (3.1 mg/dL), which was consistent with the information that younger men generally had better insulin sensitivity[35]. This variant underscores the role of reduction in refined carbohydrate and other dietary changes in reducing fasting glucose[36].
This FBS decrease was significant in all participants categories, demonstrating the effectiveness of dietary and lifestyle modifications in controlling blood glucose even in older men and the elderly[37]. These data add further support for the role of dietary interventions and physical activity in the management of FBS levels in subjects with different degrees of insulin resistance.
3.3 Change in Glycosylated Haemoglobin (HbA1c) across age groups in Female subjects
Glycosylated Haemoglobin (HbA1c) reductions for females aged 30-40 years: 0.2% from 5.9% to 5.7%) are more pronounced than those of older females (40-50 and 50-60 years). The 50-60 female group showed no change in Glycosylated Haemoglobin (HbA1c) as opposed to the males, implying that hormonal factors (e.g., in this case estrogen drop) had an effect on glucose homeostasis[34] and also indicates that older women may need more intensive measures, including possible pharmacotherapy.
Findings indicate that premenopausal women (younger age groups) tend to exhibit more positive responses to lifestyle interventions, potentially because of younger age groups, which maintain higher levels of estrogens augmenting insulin sensitivity[37].
Structured meal planning and reduction of visceral fat have been shown to elicit a strong treatment effect in the middle-aged adult population[32] which further suggests its strong potential for the field implementation. Higher baseline Glycosylated Haemoglobin (HbA1c) in females may associate with metabolic changes during the perimenopause, as shown[38], partially reduced by dietary interventions.
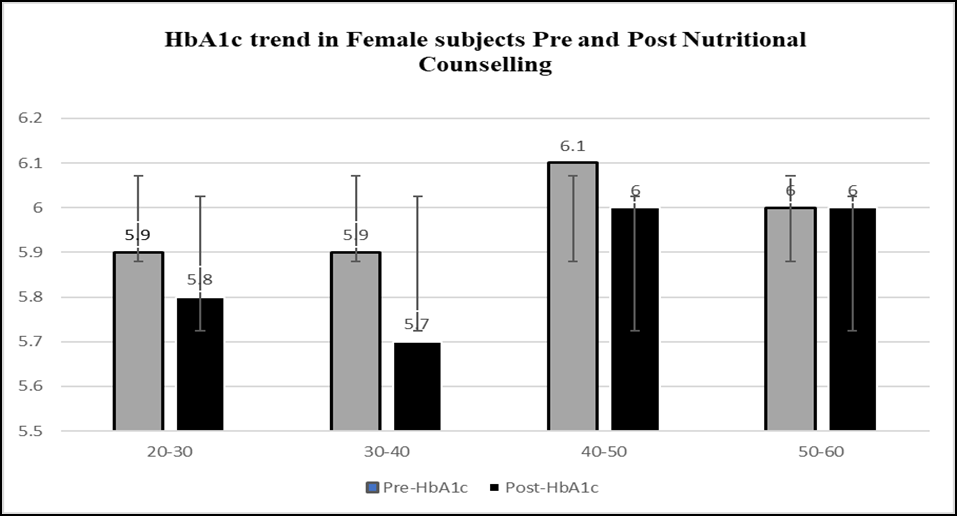
Note: This graph depicts Glycosylated Haemoglobin (HbA1c) levels before and after intervention across different age groups in female subjects. Error bars represent standard deviation.
3.4 FBS Reduction in Females across all age groups
FBS was reduced in all age group and the most reduction in the 30-40 groups (5.5 mg/dL, from 99.6 to 94.1 mg/dL). For the age categories of 40-50 and 50-60, the decrease in FBS is far less than for male patients, corroborating similar findings on the higher insulin resistance in postmenopausal departments arising from changes in hormones[35].
Females presented with lower reductions in FBS than males with much of the distinction evinced in older age groups (50-60 years); this difference was observed to be negligible in the younger demographic and can be explained as hormonal fluctuations (post-menopause) working to bestow protection against hyperglycaemic states[34].
Despite moderate reduction of FBS in all age brackets, females in older age brackets appeared to have slower improvement in glucose levels compared to males which could be attributed to age-related metabolic changes[33].
| Age Group | Pre-FBS (mg/dl) (Male) | Post-FBS (mg/dl) (Male) | Pre-FBS (mg/dl) (Female) | Post-FBS (mg/dl) (Female) |
|---|---|---|---|---|
| 20–30 | 95.2 ± 7.1 | 92.1 ± 4.5 | 98.5 ± 9.7 | 94.3 ± 6.5 |
| 30–40 | 100.4 ± 9.5 | 94.7 ± 4.8 | 99.6 ± 8.2 | 94.1 ± 4.3 |
| 40–50 | 104.2 ± 13.0 | 95.8 ± 7.2 | 101.3 ± 11.1 | 96.2 ± 5.9 |
| 50–60 | 105.8 ± 9.8 | 96.5 ± 6.4 | 98.7 ± 10.5 | 95.4 ± 5.3 |
| Parameter | Baseline (Mean ± SD) | Post-Intervention (Mean ± SD) | Δ (Mean ± SD) |
|---|---|---|---|
| HbA1c (%) | 6.0 ± 0.3 | 5.8 ± 0.4 | −0.2 ± 0.1* |
| FBS (mg/dl) | 108.5 ± 12.1 | 98.7 ± 10.9 | −9.8 ± 8.5* |
*p* < 0.001 for all parameters (paired t-test).
4 Discussion
The pre -intervention and post-intervention data shows a statistically significant improvement in the Glycosylated Haemoglobin (HbA1c) and FBS levels across all age-groups and both the gender groups. The persistent decline in both parameters highlights the positive impact of lifestyle changes, although the extent of improvement seen in parameters is influenced by metabolic aspects of age and gender.
4.1 Changes in Glycosylated Haemoglobin (HbA1c) Levels
Glycosylated Haemoglobin (HbA1c), a robust long-term measure of glucose control, demonstrated a statistically significant reduction among both males and females, corroborating the strength of structured dietary and lifestyle interventions. However, pre-intervention Glycosylated Haemoglobin (HbA1c) levels were modestly higher in the older patients, indicating a background of increasing insulin resistance with age[33].
Glycosylated Haemoglobin (HbA1c) decreased from 6.1% to 5.9% in males and from 6.0% to 5.8% in females. The greatest reduction was seen in the younger (20-40 year)-age groups, due to better insulin sensitivity[32] and metabolic flexibility. The older participants (50-60 years) had a modest reduction, as expected due to age-related metabolic adaptations and increased insulin resistance[39].
The greater reduction in Glycosylated Haemoglobin (HbA1c) seen in females than in males (especially in younger groups) indicates a protective role of oestrogen on glucose metabolism, which is diminished after menopause[37].
Glycemic control improved, with a −0.2% reduction (*p* < 0.001), moving participants closer to the normal range (<5.7%).
These findings align with prior data that show that lifestyle interventions are most efficacious in younger adults and those with higher baseline Glycosylated Haemoglobin (HbA1c)[2]. However, older people still get great benefits, although to a lesser extent due to progressive β-cell dysfunction[34].
Our finding that women, particularly premenopausal participants, experienced greater HbA1c reductions aligns with recent secondary analyses of large prevention trials, which attribute these differences to estrogen-mediated effects on insulin sensitivity[6]. The modest response in postmenopausal women further supports the need for adjunct strategies, as highlighted in recent menopause-focused intervention studies[7]. Moreover, the success of our remote, digitally-monitored intervention is consistent with current evidence affirming the efficacy of tele-nutrition in managing prediabetes[23].
4.2 The Variation of Fasting Blood Sugar (FBS) Levels
The FBS as an indicator of short-term glycaemic control also significantly decreased in all subjects. The decrease was more pronounced in males than females, suggesting an underlying metabolic difference influencing glucose regulation during fasting based on gender[35]. The overall FBS reduction in males was higher (by 8-9 mg/dL on average) than that in females (4-6 mg/dL).
The largest reduction (-8.4 mg/dL) was observed in the 40-to-50-year group suggesting that individuals with higher FBS levels at the start may receive greater benefit from lifestyle intervention[33].
Females presented with lower reductions in FBS than males with much of the distinction evinced in older age groups (50-60 years); this difference was observed to be negligible in the younger demographic and can be explained as hormonal fluctuations (post-menopause) working to bestow protection against hyperglycaemic states[34].
Older females show less pronounced improvement, highlighting the potential requirement for complementary interventions, such as specific dietary adjustments or hormonal treatments, to further enhance glycaemic control[37].
These findings align with recent investigations into age- and gender-specific responses to lifestyle modification. A 2023 meta-analysis confirmed that younger adults and women of premenopausal age exhibit more pronounced improvements in HbA1c following structured dietary interventions[5]. Additionally, studies focusing on the postmenopausal population suggest that integrating resistance training with dietary counselling may yield better glycaemic results than dietary changes alone[40].
FBS decreased by −9.8 mg/dl (*p* < 0.001), indicating enhanced insulin sensitivity. The results are consistent with evidence that fasting glucose levels are generally more amenable to intervention in a population more compatible with insulin resistance[2]. Moreover, men typically start with a higher fasting glucose compared to women and thus are more prone to show greater improvements from dietary and physical activity changes[35].
4.3 Implications for Practice and Future Directions
In younger populations, intensive lifestyle interventions are very effective in improving glycaemic parameters, supporting the rationale behind screening and prevention of diabetes mellitus at younger ages. In older people, especially postmenopausal women, additional therapeutic approaches like pharmacological aid or specific nutritional solutions may be needed to get desired glycaemic results.
Moreover, male participants experienced larger decreases of FBS while female participants benefited in terms of Glycosylated Haemoglobin (HbA1c), indicating the possibility of gender as a component for the metabolic approach when addressing diabetes.
The observed reduction in both Glycosylated Haemoglobin (HbA1c) and FBS level corroborate the significance of lifestyle modifications in the progression of prediabetes to diabetes where even a moderate change can have a long-lasting effect on improving metabolic syndrome.
Additional studies examining hormonal fluctuations, body mass, and personalized approaches for intervention should be conducted to improve glycaemic outcomes in various populations.
5 Conclusion
This study demonstrates the effectiveness of lifestyle modification and glycaemic control in improving the diabetes status from a comprehensive study of adolescent, adult, and mixed-gender populations. They had significant reductions in Glycosylated Haemoglobin (HbA1c) and fasting blood sugar (FBS) levels, with younger people being more responsive to the interventions. Male subjects were seen to have a more significant reduction in FBS when compared to females, while females experienced a more significant reduction in Hb1Ac, especially in early age and premenopausal patients. The findings highlight the importance of stopping prediabetes early, since younger individuals with more insulin sensitivity reacted better.
However, the modest improvements in older adults, particularly postmenopausal women, indicate a need for additional therapeutic strategies, beyond lifestyle changes, to address these parameters in this population. These findings highlight the relevance of age- and gender-specific diabetes prevention strategies to optimize glycaemic exposure and mitigate type 2 diabetes risk. Long term sustainability of these interventions and generalisation to metabolic health should be assessed in future study.